
Breast imaging could reduce false positive examinations
Seno Medical Instruments, Inc. has announced positive data from PIONEER, a Phase III pivotal trial of its Imagio breast imaging system. The study found that OA/US was more specific than device gray-scale ultrasound alone (US) in differentiating malignant from benign breast lesions and was non-inferior to US with respect to sensitivity. This means that OA/US detected a similar number of malignant lesions as US but had a lower rate of false positive malignant diagnoses.
These data were highlighted during an oral presentation by a principal investigator involved with the study at the Radiology Society of North America 103rd Annual Meeting, taking place November 26 – December 1 in Chicago.
PIONEER was a U.S., prospective, multi-institutional study that enrolled 2,105 women over the age of 18 years. All participants had a breast mass assessed by initial conventional site ultrasound as BI-RADS (Breast Imaging and Reporting Data System, or BR) category 3, 4, or 5.

The likelihood that a breast mass is malignant increases with increasing BR category number. Radiologists at each clinical site also assigned each mass a probability of malignancy (POM) ranging from 3% to 99% based on mammographic and US features.
Patients with masses categorised as > BR4A had OA/US prior to undergoing core needle biopsy within 45 days of their initial visit and subsequent biopsy or excision surgery within 45 of the initial biopsy. Patients with BR3 masses had OA/US upon enrollment and underwent biopsy or conventional site US and OA/US 12 months after enrollment.

Patients who underwent biopsy due to new clinical or imaging findings within the 12-month period had additional OA/US imaging within 45 days prior to the biopsy.
Independent breast imagers who were blinded to the biopsy and other clinical information read the OA/US and device US images; an independent central pathologist who was blinded to the imaging data reviewed all of the biopsy reports.
Key findings from the study include:
- Seven independent readers blinded to clinical and biopsy information conducted 12,283 mass reads.
- In the intent to diagnose (ITD) population 1808 masses were evaluated in 1,739 subjects (678 malignant, 889 benign, 190 benign with 12-month follow-up).
- In the ITD population of 1,739 subjects and 1,808 masses, diagnostic specificity for benign masses was 43% for OA/US and 28.1% for US, corresponding to a 14.9% absolute specificity advantage for OA/US over US (p<0.0001).
- Subgroup analyses showed no significant differences in specificity for either OA/US or US based on breast density, mass size, palpability, distance from nipple and depth.
- Specificity of OA/US was 8.4% higher in patients <50 years of age than in patients aged 60 to <70 years; there was no difference in sensitivity by age group.
- For masses that were benign, OA/US resulted in downgrading 34.5% of US reads (from BR4A to <BR3 or BR3 to BR2). OA/US also resulted in upgrading 6.0% of US mass reads, for a net downgrade rate of 28.5% (p<0.0001).
- For masses that were malignant, OA/US resulted in upgrading 47.0% of mass reads classified as BR3 by US and downgrading to BR2 27.3% of mass reads classified as BR3 by US.
- Positive predictive value for masses assessed as BR4A or higher was 51.5% for OA/US compared with 46.3% for US; negative predictive value for masses assessed as BR3 or lower is 94.4% for OA/US compared with 97.0% for US.
- Ten patients reported 11 adverse events potentially related to the OA/US procedure, all of which were considered mild and resolved within a few days (7 paresthesias, 1 erythema, 1 warmth, 1 tenderness and 1 case of possible dermatitis of indeterminate origin).
"These data demonstrate that OA/US improved diagnostic specificity compared with US, resulting in reclassification of both benign and malignant lesions," said Erin Neuschler, M.D., Assistant Professor of Radiology at the Northwestern University Feinberg School of Medicine and the co-principal investigator of the PIONEER study.
"The ability to downgrade the BI-RADS assessment of some benign masses may lead to fewer false positive examinations, short-term interval follow-up studies, and benign biopsies, potentially improving the accuracy of the diagnostic work-up and reducing some of the limitations and perceived harms of breast imaging."
"This pivotal trial supports the Imagio system as an important advancement in evaluating breast masses and more accurately differentiating malignant and benign lesions," said Tom Umbel, CEO of Seno Medical Instruments. "OA/US offers patients and clinicians an alternative diagnostic method that may increase specificity without significantly impacting sensitivity.
False positive examinations and negative biopsies increase women's anxiety, pain and radiation exposure, and are a contributing factor in non-compliance with current breast cancer screening recommendations. The Imagio OA/US system shows the potential to positively affect these concerns and reduce healthcare costs in the process."
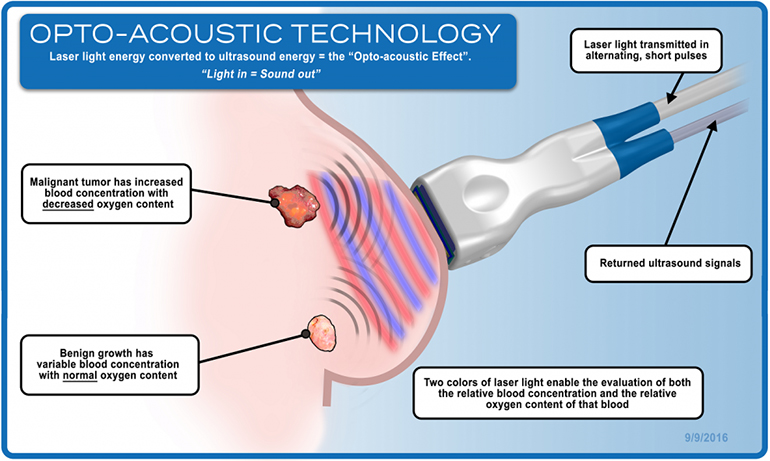
The Imagio breast imaging system was designed and is being studied to identify two functional hallmarks of cancer: the presence of abnormal blood vessels (tumor angiogenesis) and the relative reduction in oxygen content of blood that occurs in cancer compared to benign masses and normal tissues. The technology is CE marked in Europe and the subject of a U.S. PMA filing with the FDA.

Featured products

MAX17793
Analog Devices Inc.
3V to 80V, 3A, High-Efficiency, Synchronous Step-Down DC-DC Converter
| SKU: | MAX17793 |
|---|---|
| Stock: | 9316 |
| Cost: | $3.64 |

MAX22516
Analog Devices Inc.

IO-Link Data Link Controller with Transceiver and Integrated DC-DC
| SKU: | MAX22516 |
|---|---|
| Stock: | 8000 |
| Cost: | $5.42 |
Product Spotlight
102991834
BeagleBoard

Single Board Computer (SBC), BeagleY-AI
AM67A BeagleY-AI Jacinto 7 AR...
| SKU: | 2820-102991834-ND |
|---|---|
| Stock: | 206 |
| Cost: | $56.24 |
SC1110
Raspberry Pi
Raspberry Pi 5 2GB
The Raspberry Pi 5 2GB model represents a leap for...
| SKU: | 2648-SC1110-ND |
|---|---|
| Stock: | 0 |
| Cost: | $38.33 |
AKX00069
Arduino
Arduino Plug and Make Kit
The Arduino Plug and Make Kit features the ...
| SKU: | |
|---|---|
| Stock: | 968 |
| Cost: | $66.97 |
300361-0011
Molex
MX150 Mid-Voltage MatSealed Female Connector Assembly, Dual Row, 20 Circ...
| SKU: | |
|---|---|
| Stock: | 280 |
| Cost: | $2.51 |